
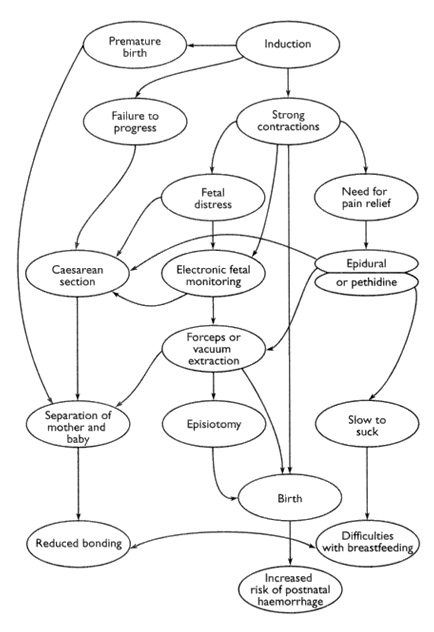
Cascade of Interventions Following Induction
from anthrodoula.blogspot.ca
According to Perinatal Services of BC, induction rates vary widely across the province and have been risen substantially since the early 90’s. . In 1991, 12.9% of births were induced, and by 2000 the rates were up to 27.2%. Current estimates continue to sit at around 25%.
This is a very high percentage! Induction of childbirth is often part of what childbirth professionals all the “Cascade of Interventions“. According to the Royal College of Midwives in the UK,”The adverse effect of the injudicious use of induction is the possible triggering of the so called “domino” or “snowballing” phenomenon of increased intervention, which could end in emergency caesarean section if induction fails.”
Optimal Birth BC states that the most common reasons for induction are “pregnancy extending beyond 40 weeks and prolonged prelabour rupture of membranes. Induction of labour is associated with increased cesarean section rates among first time mothers.”
The reason given for inducing childbirth for being post-dates is the hope of minimizing risk of still-birth. However, induction is a very serious procedure that comes with many risks, and there is controversy about whether or not any of its potential benefits outweigh those risks.
Resources for understanding why women are starting to decline routine induction based on being postdates (“overdue”):
Reducing Inductions: Lack of Justification to Induce for Post-Dates: an excellent paper by Judy Slome Cohain on why induction for being post-dates, or “overdue” may not be the best practice:
Excerpt 1: Drawbacks of routine induction include: a 13% increase in premature births between 34–36 weeks, no improvement in perinatal mortality, no documented decrease in stillbirths (except in low-level studies), no research showing safety as regards immediate and long term brain function, 5% increase in the elective cesarean rate, a possible increase in brachial palsy, no decrease in meconium aspiration syndrome and two to three times more maternal deaths or near misses from amniotic fluid embolism.
Excerpt 2: Two thousand women would have to be treated to prevent one still-birth at 41 weeks and the treatment would have to be one that does not increase perinatal mortality itself. Would inducing 2000 women at 41 weeks prevent one stillbirth? So far, there is a lack of quality evidence to indicate that this is the case. Two reviews found no significant difference in perinatal mortality including stillbirths between induction and expectant management groups (Sanchez-Ramos 2003; Gülmezoglu and Crowther 2006). Systematic induction before 42 weeks has not been shown to lower the perinatal mortality or stillbirth rates (Zeitlin et al. 2007). There is no high-quality research clearly supporting induction at 41 weeks.
Excerpt 3: Does stillbirth increase significantly after 42 weeks? Yes. However, induction of labor has not been shown to significantly decrease stillbirth or overall perinatal mortality.
Risks of induction according to the Society of Obstetricians & Gynaecologists of Canada:
Potential risks of induction include increased rate of operative vaginal delivery, Caesarean birth, excessive uterine activity, abnormal fetal heart rate patterns, uterine rupture, maternal water intoxication, delivery of preterm infant due to incorrect estimation of dates, and possibly cord prolapse with artificial rupture of membranes
*Note the risks here, such as operative vaginal delivery, caesarean birth and abnormal fetal heart rate patterns themselves have further risks to both mother and baby.
Check out the BC Midwifery Guidelines on Management of Uncomplicated Postdates Pregnancy.
Here are some great blog posts discussing opinions on induction:
Post By: Jessica Austin: Childbirth support and information in Vancouver, BC
Don't miss out on other original childbirth articles like this one! Join other mothers and birth professionals on my mailing list!